Article Text

Abstract
Scientific and public interest relating to golf and health has increased recently. Players, potential players, the golf industry and facilities, and decision makers will benefit from a better understanding of how to realise potential health benefits and minimise health issues related to golf. We outline an International Consensus on Golf and Health. A systematic literature review informed the development of a survey. Utilising modified Delphi methods, an expert panel of 25 persons including public health and golf industry leaders, took part in serial surveys providing feedback on suggested items, and proposing new items. Predefined criteria for agreement determined whether each item was included within each survey round and in the final consensus. The working group identified 79 scientifically supportable statement items from literature review and discussions. Twenty-five experts (100%) completed all three rounds of surveys, rating each item, and suggesting modifications and/or new items for inclusion in subsequent surveys. After three rounds, 83 items achieved consensus with each with >75% agreement and <10% disagreement. These items are included in the final International Consensus on Golf and Health. The final consensus presented here can inform scientific knowledge, and action plans for (1) golfers and potential golfers, (2) golf facilities and the golf industry, and (3) policy and decision makers external to golf. These outputs, if widely adopted, will contribute to an improved understanding of golf and health, and aid these groups in making evidence-informed decisions to improve health and well-being.
- golf
- public health
- physical activity
- sport
- consensus
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Introduction
Recent consensus statements related to sport and health have provided comprehensive, evidence-informed summaries of key issues1–3 to help people make informed decisions, and to guide implementation.4
Golf is a sport played by over 60 million people on six continents.5 6 There has been a recent increase in scientific and public interest relating to golf and health with a decade on decade increase in scientific papers and their uptake.7 8 Our 2016 systematically conducted scoping review7 and others9 have highlighted that golf can provide moderate-intensity physical activity, and may be associated with longevity,10 physical health11 12 and wellness benefits.13 14 Conversely, negative health outcomes including injury15 16 and an increased risk of skin cancer17 have been associated with playing golf.
The need for a comprehensive, evidence-informed consensus summary of key issues, and key actions with regard to golf and health was recognised by the World Golf Foundation and its constituent members who are golf’s global leaders.
The objectives of this study are:
To engage leaders at the intersection of health, sport, policy and golf to build a cross-sectoral agreement relating to golf and health.
To achieve consensus on (1) the health risks and benefits associated with golf, (2) how individuals and populations can improve their health through playing golf or spectating at events, (3) how the golf industry and (4) policymakers can increase opportunities for gaining health benefits through golf and minimise the health risks of golf.
This consensus will enable players, potential players and spectators to benefit from knowledge of how to realise health benefits, and minimise associated health risks related to golf. It will facilitate policymakers to raise awareness and support potential public health interventions, and the golf industry to support education and best practice.
Methods
The consensus was reached by use of the Delphi method. This is a well-accepted, rigorous and systematic method for achieving consensus of opinion among experts and identifying priorities on real-world issues.18 These methods can assist in drawing on the best available evidence, and the opinions and experiences of individuals and the organisations they represent. Methods developed by Dalkey and Helmer19 have been refined and adapted for a range of settings including healthcare, sport and policy.20–27 The Appraisal of Guidelines for Research and Evaluation 228 instrument was used to inform the conduct of this study.
Preliminary work: literature review and framework development
A working group of five individuals with expertise in public health, golf and health, policy, industry and research methods was established to facilitate the Delphi consensus process. Preliminary work was conducted by the working group who updated a 2016 systematic search (screening a further 669 relevant records), and extracting further data as shown in figure 1.7 8 Relevant guidelines and policy documents were reviewed, and discussions with authors of primary studies and reviews, and other leading authorities were conducted where clarification was helpful.

Literature review flow diagram.
A framework for organising the available evidence for building a golf and health consensus was developed. Each domain/heading was populated with potential items for inclusion in the proposed survey. A draft survey was generated using Survey Monkey (San Mateo, USA), which was assessed for content and form by the working group and three additional researchers with expertise in public health.
Selection of expert panel
To maximise objectivity in expert panel selection, it was determined to invite all 25 contributors to the 2018 International Conference on Golf and Health, a satellite meeting of the International Society of Physical Activity for Health 2018 conference. These individuals had an expertise in one or more of (1) public health/physical activity for health policy, (2) the golf and health subject area, and (3) the golf industry. Potential expert panel members were sent an email introducing the concept, and providing a participant information leaflet. Consent was gained electronically.
Rounds of Delphi survey
Round 1
An initial questionnaire with proposed items for the consensus based on the preliminary work of the working group was circulated to the expert panel. Each was invited to grade each item on a five-point Likert scale29 (‘strongly agree’, ‘agree’, ‘neither agree nor disagree’, ‘disagree’ and ‘strongly disagree’), and to suggest items and make comments that they thought would add value to the next iteration of the questionnaire. It was stated that the level of evidence for items was variable, and that expert panel input was encouraged. The survey results were collated by the working group.
Round 2
The anonymised results from round 1 were fed back to the panel allowing members to appreciate the opinions of others, and the reasons for their position.26
Cut-offs for levels of agreement at each round were defined ‘a priori’ following working group discussion. In round 1, items scoring >65% agreement (agree or strongly agree) were included in the questionnaire for round 2. In keeping with established practice, modifications to existing items were incorporated by the working group following review of all expert panel comments from survey 1,18 while additional items suggested during round 1 were discussed by the working group and where agreed added to the questionnaire. The 25 original experts were then invited to take part in a second round survey. Participants were invited to rescore each item on the Likert scale, and provide additional comments.
Subsequent rounds
Items scoring agreement of >75% in round 2 were included for round 3. Final consensus was defined as items scoring agreement (agree or strongly agree) in 75%,25 27 and disagreement (disagree or strongly disagree) in <10% of respondents. The survey process was repeated until consensus had been reached (stability of existing items meeting criteria >85% of items)24 and no new items requiring inclusion.
Data analysis
The results of each survey were exported from the Survey Monkey Platform to Excel (Microsoft, Washington, USA). Stacked leaning bar charts (Peltier Tech Advanced V.3.0) were used to present data. A summary of methods is shown in figure 2.
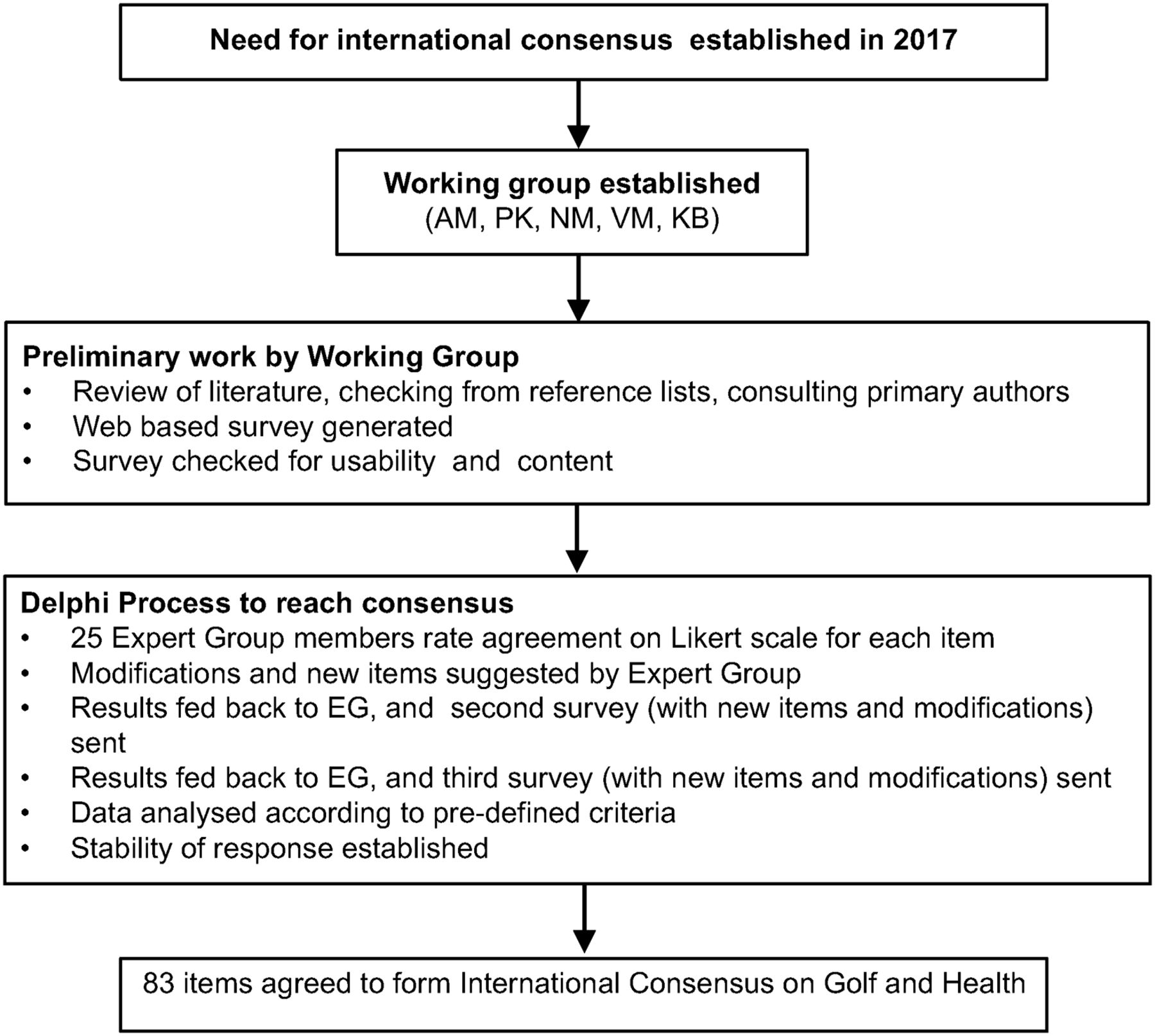
Summary of methods used to develop an International Consensus on Golf and Health. AM, Andrew Murray; EG, expert group; KB, Kevin Barker; NM, Nanette Mutrie; PK, Paul Kelly; VM, Valerie Melvin.
Results and discussion
Literature review and framework development
The literature review identified 5605 records. After (1) screening of articles, (2) exclusion of duplicates, (3) further identification of studies through review of references (‘snowballing’) and (4) consultation with subject area experts, 342 articles had data extracted to inform the proposed International Consensus on Golf and Health.
Review of all data sources and working group discussions generated 79 statements/items emerging from the data which were categorised into three broad domains:
Domain 1: Golf’s associations with health and potential mechanisms.
Domain 2: Correlates, determinants, diversity and sustainability.
Domain 3: Interventions and knowledge transfer.
These were further subcategorised as per table 1.
A framework for building a golf and health consensus
Establishing consensus using Delphi methods
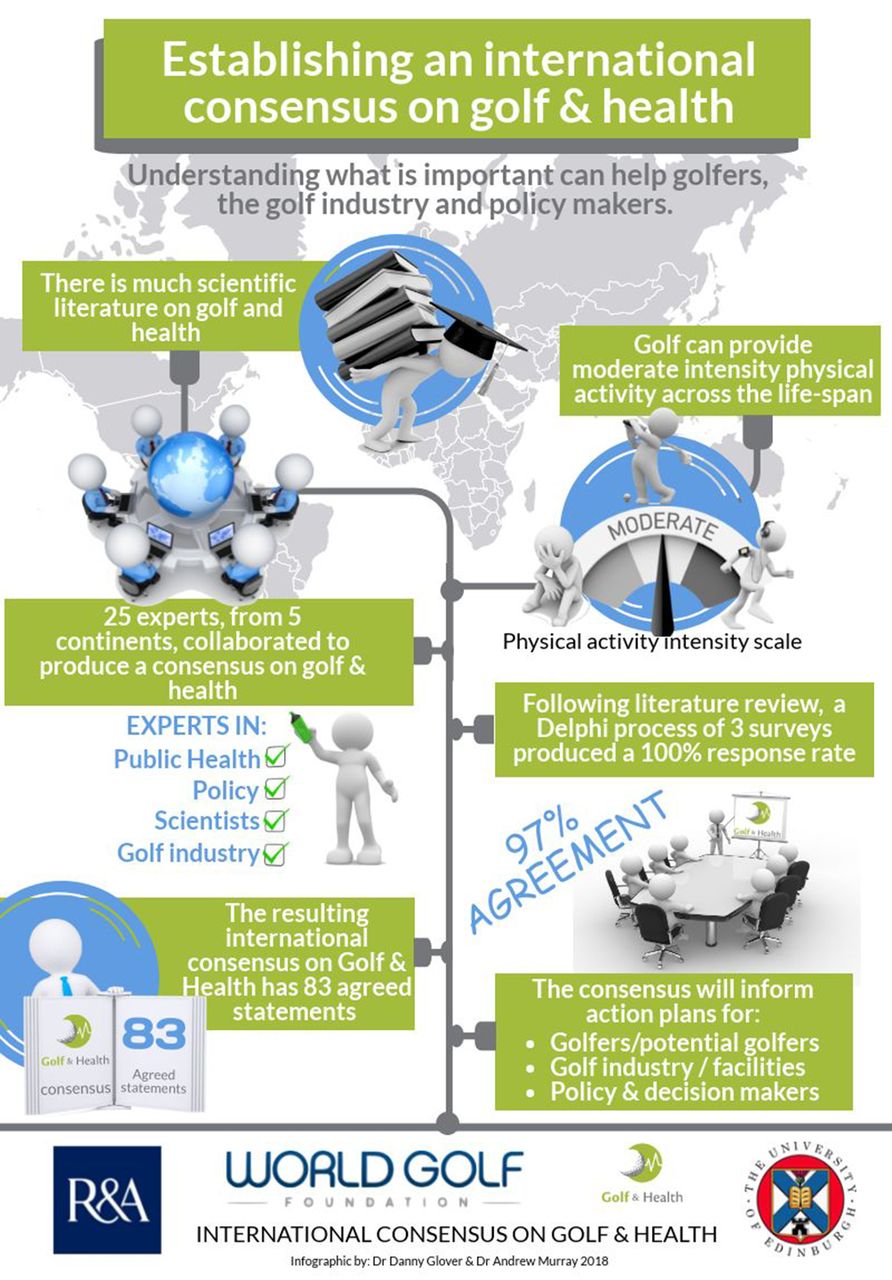
The results from each round of survey are summarised in table 2. Twenty-five members of the expert group completed each of the three serial surveys within the allocated time frame (a 100% response rate). Following round 1, six new items and 21 modifications were incorporated for survey 2. Following round 2, two new items and 17 modifications were included for round 3. Three iterations or ‘rounds’ of survey were sufficient to collect the required information and reach consensus by predetermined criteria.18 26
Summary of results at completion of each survey round in the Delphi process to establish an International Consensus on Golf and Health
Agreement (defined by >75% ‘agree’/‘strongly agree’ and <10% ‘disagree’/‘strongly disagree’) was achieved for each and all (100%) of 83 individual items included within survey 3. Across all the items, the mean percentage of expert panel that agreed or strongly agreed with statements was >97%.
A summary of processes establishing the consensus are shown in figure 3. All items reaching consensus are shown in table 3, with further detail provided in supplementary file 2.

Visual summary of processes establishing an international consensus on golf and health. AM, Andrew Murray; EG, expert group; KB, Kevin Barker; NM, Nanette Mutrie; PK, Paul Kelly; VM, Valerie Melvin.
Final consensus statements and levels of agreement
Summary of consensus
We aimed to establish a consensus on what is known based on the best available scientific evidence and identified 83 items covering three principle domains by Delphi process. The 25 expert panel members provided representation in global public health and sustainability, physical activity for health, health and sport policy, and included clinicians/academics with golf and health subject knowledge. Senior leaders/accountable officers from the World Golf Foundation, The R&A, the European Disabled Golf Foundation, golf facility managers and professional organisations representing golf coaches internationally provided an industry context vital for the building of consensus, but importantly also for the ongoing engagement of stakeholders able to collaborate and deliver evidence-informed decisions and interventions to improve health and well-being in relation to golf.
Three principal domains were identified within the consensus with critical elements discussed below.
Domain 1: golf’s associations with health and mechanisms
This domain included 25 statements, with over 90% of the expert panel agreeing with each item. These statements describe health benefits/disbenefits of golf, the mechanisms by which benefits are achieved, and the volume and intensity of participation needed for these benefits.
Relationships of golf with health outcomes
The best available evidence reports golf can have overall health benefits,7 30 31 being associated with increased longevity10 32 and improving known risk factors for cardiovascular disease.11 12 33 34 Golf is associated with mental well-being benefits,31 35–40 and can positively influence health for those with disability.31 41 Compared with other sports, the annual risk of injury is moderate,15 while golfers may be exposed to increased risk of skin cancer.7 17 The magnitude of health benefits will depend on many factors including age, gender, genetic factors, and the existing fitness/wellness of the participant, the topography of the course and the frequency of play.7 While a significant body of evidence exists relating to golf and health, further high-quality research is needed to assess relationships between golf and mental health, benefits to particular populations, and to explore cause and effect relationships between golf and health.7 31 42
Mechanisms to achieve health outcomes
Golf can provide social interaction,38 42–45 health-enhancing physical activity,33 green exercise and nature connection for persons of all ages,31 42 45 46 and specifically can provide moderate-intensity aerobic physical activity.7 33 Strength and balance benefits are likely for older adults,47–49 while further research is needed to assess strength and balance benefits for wider populations.7 Health benefits are likely greater for those walking the course as opposed to riding a golf cart, although those playing and riding a cart do gain health benefits.7 33 Taking part in physical activities additional to golf is likely to offer further health gains.50 Spectating in an active fashion (eg, walking the course) at golf courses/tournaments offers an opportunity for health-enhancing physical activity.51 52
Dose and effect
Adults should meet WHO recommendations for physical activity.53 54 Participation in golf/other physical activities over and above the minimum guidelines is likely to offer additional benefits.7 50 Being physically active/playing golf regularly throughout life provides greater benefits than being active/playing golf intermittently.
Domain 2: correlates, determinants, diversity and sustainability
This domain included 14 statements that describe who plays golf, what helps or hinders participation, and covers sustainability considerations with respect to golf. Knowledge regarding patterns of participation and determinants is critically important in helping maximise interest and participation in a sport with well-accepted overall health benefits. Golf’s global leadership including The R&A, and the World Golf Foundation have identified challenges related to sustainability including improving diversity of participation, but opportunities to contribute positively and collaboratively towards the United Nations Sustainable Development Goals 2030.31 46 55 56
Behavioural patterns/participation
Over 60 million people have played golf twice or more in the previous year.5 Participation is currently highest in North America, Australasia and Europe, and in in men compared with women, in middle-aged and older adults, in some ethnic groups (White-European heritage) and in those of middle and higher socioeconomic class.56–59 Over 20% of adults globally do not meet the WHO Global Recommendations on Physical Activity for Health.53 60 Sports programmes that encourage participation across the lifespan have been recognised as an approach that can work to positively impact physical activity.61 62
Correlators and mediators
To increase participation in sport, there is a need for an inclusive environment that embraces, encourages and welcomes individuals, groups and families from all of society,31 42 46 62 and this is true of golf.31 46 56 57 Efforts to provide an infrastructure, social norms and regulations that are welcoming to all can lower barriers to participation.31 46 63 Some factors that help interest and participation in the sport are that golf can (1) be enjoyable, (2) be played throughout life, (3) offer a sense of community, (4) offer challenge and/or competition, (5) provide outdoor exercise and (6) provide time for self.31 56 57 63 Golf can also teach life skills,45 while facilities can provide a social/community hub.31
Some factors that may hinder interest and participation in the sport include perceptions that it is expensive, less accessible for those from lower socioeconomic groups, male dominated, a sport for older people, or difficult to learn.31 56 63 The cost of playing golf can hinder participation in some countries and at some facilities, while other facilities do offer affordable opportunities. Not everyone will be attracted by the same things at a golf facility, so diversity and specialisation of golf facilities in keeping with the local context, culture and population is appropriate.
Golf and sustainability
Promoting regular physical activity can support the attainment of a number of the United Nations Sustainable Development Goals.64 This consensus recognised the importance of supporting international policy31 54 55 64 and best practice in this regard. Golf can work to promote sustainability through practices that prioritise diversity, healthy societies, connection with and care of the environment, environmental integrity, and health and well-being.31 42 45 46 57
Domain 3: interventions and knowledge transfer
The third domain contains 42 individual items, highlighting its fundamental importance. This section explores what interventions work in promoting golf, and what can practically and feasibly be done to maximise health benefits and minimise health risks associated with golf. The weight of evidence is generally weaker than for other categories, with some recommendations based on consensus of opinion. Practical actions, building on existing progress, can help increase physical activity.61 62 65
Included are 13 actions for golfers/potential participants, 18 actions for golf facilities/the golf industry and 10 actions for policy/decision makers external to the golf industry that if widely disseminated and adopted will contribute to an improved understanding of golf and health, and aid these groups in making evidence-informed, more consistent decisions and interventions to improve health and well-being. Representatives from these groups have been key in making these recommendations. These are summarised in the section below, and in table 3. Bite-sized assets (infographics, podcast and video; Murray AD, Infographics and digital resources. An international consensus on gold and health. Under peer review) for golfers, the golf industry and facilities, and policy/decision makers have been produced to facilitate uptake by these groups.
Interventions
Appropriate partnerships within, and outwith the sport sector can support interventions to make the sport more inclusive and welcoming.31 42 45 46 57 Interventions are required to increase access and participation, building on theories around engagement, enjoyment, and including effective monitoring and evaluation aspects.
Actions for golfers/participants
Golfers should aim to play golf at least 150 min/week,7 53 or engage in other forms of moderate to vigorous physical activities additional to golf. Golfers can be encouraged to walk the course, as opposed to riding a golf cart if able.7 66 Warming up with some aerobic exercise (eg, stair climbing or stationary bike), then golf-specific mobility exercises, then practice swings can help maximise performance and minimise injury risk, as can appropriate strength and conditioning.67 68 Golfers should be encouraged to make others feel welcome, and support others to enjoy golf.31 42 Spectators at golf tournaments can be encouraged to walk, and spectate in an active fashion.
To minimise health risks, golfers should follow appropriate lightning69 and golf cart safety guidelines.70 Golfers should use sunscreen and appropriate clothing (collared shirt, hat, and so on) as appropriate,71 and moderate exposure to direct sunlight.72 Children should be adequately supervised.7 Golfers with cardiovascular disease can play with acceptable safety, but should see a doctor should symptoms increase or be unstable.7 Golfers can be expected to return to golf following total knee, hip or shoulder replacement, with a graduated return to golf.73
Actions for golf facilities/the golf industry
Recommendations are presented for golf facilities and the golf industry. The World Golf Foundation and The R&A who lead golf development activity globally are committed to working with a range of stakeholders to deliver and support key actions related to golf and health, and communicate key actions to the 60 million golfers worldwide.
Grass-roots initiatives supporting development of golf in regions/countries where golf is a relatively new sport can help encourage growth in these areas.6 45 56 Golf facilities and the golf industry should build on existing initiatives promoting inclusivity, and encourage increased participation by developing environments and price structures that are welcoming to all.31 42 45 57 The golf industry/golf facilities can encourage and facilitate regular physical activity, other health-enhancing behaviours (eg, healthy eating), and counsel about the dangers of excessive sun exposure. Practices that enhance sustainability, including maximising opportunities for wildlife conservation, interaction with green space, restricting water, energy and pesticide/chemical use, should be encouraged.42 56
Golf facilities and other golf industry leaders and stakeholders can commit and can work together to develop an environment that will inspire and recruit more women and girls to play golf, and retain their participation in the game.46 56 Effective learning and coaching environments, and entry-level play, can be further encouraged, with facilities considering the preferences of the average golfer.63 Facilities should make every effort to promote equality and diversity, and make golf accessible and environmentally sustainable.42 Facilities should consider being multifunctional (having facilities in addition to golf; eg, gym, walking routes or child care) and having diversity of golf facilities.42
Further, facilities should be encouraged to:
Provide information and facilities to support golfers warming up to play.
Stock sunscreen, hats and collared shirts, healthy food and water.71
Consider providing cardiopulmonary resuscitation training to staff, and provide automatic external defibrillators.7
Adequately maintain golf carts with speed limiters and front wheel brakes.
Provide appropriate lightning safety policies.
Actions for policy/decision makers (outwith the golf sector)
Decision makers at community/municipal, local, national and international levels have engaged in discussions which informed this consensus, and future delivery of plans. This consensus has considerable alignment with the WHO Global Action Plan on Physical Activity,54 and the United Nations Sustainable Development Goals.55 Further cross-sectoral collaboration can further support these global efforts. Policymakers can work collaboratively with the golf industry and national associations/federations to promote increased participation in physical activity/golf, particularly in groups with low levels of physical activity (eg, older adults).
The benefits of regular physical activity including playing golf should be communicated and promoted regularly for persons of all ages, genders and socioeconomic backgrounds. Golf can be included as a moderate-intensity7 33 physical activity in policy documents, guidance and recommendations, and participation encouraged for persons of all ages and genders. Policy documents, frameworks and actions can, where relevant, usefully acknowledge green space, health and well-being, nature connection, social and community, and local and national economic benefits of golf.31 These policies should support play by diverse geographical and socioeconomic participants, of all genders, ages and abilities, multifunctionality of facilities and sustainability considerations.
Strengths and limitations of present study
Strengths of the present study include the systematic nature of the literature review, and a 100% response rate from experts identified as leaders across public health/physical activity for health policy, the golf industry, and the golf and health subject area. Recommended standards for the conduct of Delphi studies were followed.27 This engagement in coproducing this consensus will aid collaboration in delivering the interventions and action plans that can maximise the impact of this work. We used objective criteria for expert panel selection. The level of agreement for inclusion within the consensus was high, and the threshold for excluding items low, important given the engagement with the golf industry and potential conflict of interest.
Although the search was conducted systematically, using established scoping review methodology,74 75 and some quality assessment was carried out, formal and systematic quality assessment of each study was not conducted due to the large range of subjects to be covered. The items are based on the best available evidence, and that in many cases further and more definitive research is needed. Statements contain some element of repetition, which was considered necessary by the working group for the consensus, and action plans by relevant stakeholders to be comprehensive. As evidence and practice evolves, the consensus will require revisiting and updating.
Conclusion
Our study has produced one of the first wide-ranging global consensus statements for a sport, and engaged leaders at the intersection of health, sport, policy and golf to build this cross-sectoral agreement. Consensus was achieved showing health benefits and health risks that golf is associated with, and highlighting actions by which (1) individuals and populations can improve their health through playing golf, and (2) how the golf industry/facilities and (3) policymakers can increase opportunities to gain health benefits through golf and minimise any health risks associated with golf. These outputs, if widely shared and adopted, will contribute to an improved understanding of golf and health, and aid these groups in making evidence-informed decisions and to improve health and well-being. A stacked leaning bar graph showing level of agreement for each item for survey 3 is shown in figure 4.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Stacked leaning bar graph showing level of agreement for each item for survey 3.
Supplemental material
Supplemental material
Acknowledgments
The authors thank all members of the expert panel for their enagement and commitment to the Delphi process. Members are listed in the online supplementary file 1. We thank Dr Danny Glover for designing the visual summary.
References
Supplementary materials
- bjsports-2018-099509_press-release.pdf -
Press release
- bjsports-2018-099509_press-release.pdf -
Footnotes
Contributors ADM, DA, PK, LG, IRM and NM identified the method and existing Delphi frameworks to develop this study. ADM and IRM conducted the updated search and data extraction. All authors contributed to the development of outline study design and the conduct of the study.
Funding Work for this study was supported by an unrestricted grant from the World Golf Foundation.
Competing interests ADM and RAH are supported by an unrestricted grant from the World Golf Foundation. The World Golf Foundation have agreed to publish whether the results are positive or negative for golf. RAH and ADM receive fees from the European Tour Golf for clinical work. KB is the director of Golf Development at The R&A.
Patient consent Not required.
Ethics approval School of Education, University of Edinburgh
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Further data are provided in online supplementary files. The full results of the round 1 and 2 surveys are available from the corresponding author.